 Black America Breaking News for the African American Community
Black America Breaking News for the African American Community
Related Articles
There was supposed to be a peak. But the stark turning point, when the number of daily COVID-19 cases in the U.S. finally crested and began descending sharply, never happened. Instead, America spent much of April on a disquieting plateau, with every day bringing about 30,000 new cases and about 2,000 new deaths. The graphs were more mesa than Matterhorn—flat-topped, not sharp-peaked. Only this month has the slope started gently heading downward.
This pattern exists because different states have experienced the coronavirus pandemic in very different ways. In the most severely pummeled places, like New York and New Jersey, COVID-19 is waning. In Texas and North Carolina, it is still taking off. In Oregon and South Carolina, it is holding steady. These trends average into a national plateau, but each state’s pattern is distinct. Currently, Hawaii’s looks like a child’s drawing of a mountain. Minnesota’s looks like the tip of a hockey stick. Maine’s looks like a (two-humped) camel. The U.S. is dealing with a patchwork pandemic.
The patchwork is not static. Next month’s hot spots will not be the same as last month’s. The SARS-CoV-2 coronavirus is already moving from the big coastal cities where it first made its mark into rural heartland areas that had previously gone unscathed. People who only heard about the disease secondhand through the news will start hearing about it firsthand from their family. “Nothing makes me think the suburbs will be spared—it’ll just get there more slowly,” says Ashish Jha, a public-health expert at Harvard.
Read: Georgia’s experiment in human sacrifice
Meanwhile, most states have begun lifting the social-distancing restrictions that had temporarily slowed the pace of the pandemic, creating more opportunities for the virus to spread. Its potential hosts are still plentiful: Even in the biggest hot spots, most people were not infected and remain susceptible. Further outbreaks are likely, although they might not happen immediately. The virus isn’t lying in a bush, waiting to pounce on those who reemerge from their house. It is, instead, lying within people. Its ability to jump between hosts depends on proximity, density, and mobility, and on people once again meeting, gathering, and moving. And people are: In the first week of May, 25 million more Americans ventured out of their home on any given day than over the prior six weeks.
I spoke with two dozen experts who agreed that in the absence of a vaccine, the patchwork will continue. Cities that thought the worst had passed may be hit anew. States that had lucky escapes may find themselves less lucky. The future is uncertain, but Americans should expect neither a swift return to normalcy nor a unified national experience, with an initial spring wave, a summer lull, and a fall resurgence. “The talk of a second wave as if we’ve exited the first doesn’t capture what’s really happening,” says Caitlin Rivers, an epidemiologist at the Johns Hopkins Center for Health Security.
What’s happening is not one crisis, but many interconnected ones. As we shall see, it will be harder to come to terms with such a crisis. It will be harder to bring it to heel. And it will be harder to grapple with the historical legacies that have shaped today’s patchwork.
I. The Patchwork Experience
A patchwork pandemic is psychologically perilous. The measures that most successfully contain the virus—testing people, tracing any contacts they might have infected, isolating them from others—all depend on “how engaged and invested the population is,” says Justin Lessler, an epidemiologist at Johns Hopkins. “If you have all the resources in the world and an antagonistic relationship with the people, you’ll fail.” Testing matters only if people agree to get tested. Tracing succeeds only if people pick up the phone. And if those fail, the measure of last resort—social distancing—works only if people agree to sacrifice some personal freedom for the good of others. Such collective actions are aided by collective experiences. What happens when that experience unravels?
“We had a strong sense of shared purpose when everything first hit,” says Danielle Allen, a political scientist at Harvard. But that communal mindset may dissipate as the virus strikes one community and spares another, and as some people hit the beaches while others are stuck at home. Patchworks of risk and response “will make it really hard for the public to get a crisp understanding of what’s happening,” Rivers says.
In one future scenario, the nation splinters. When national news diverges from local reality, “suspicions about whether the epidemic was a hoax will find fertile ground in places with a more ambiguous experience of the disease,” says Martha Lincoln, a medical anthropologist at San Francisco State University. Confused people will retreat to the comfort of preexisting ideologies. The White House’s baseless attempts to claim victory will further divide the already fragmented states of America. “In the face of medical uncertainty, people make decisions by returning to their own groups, which are very polarized,” says Elaine Hernandez, a sociologist at Indiana University Bloomington. “They’ll want to avoid being stigmatized, so they’ll follow what people in their networks are doing [even if] they don’t really want to go out.”
Read: Why the coronavirus hits kids and adults so differently
Prevention is physically rewarding in the long term, but not emotionally rewarding in the short term. People who stay home won’t feel a pleasant dopamine kick from their continued health. Those who flock together will feel hugs and sunshine. The former will be tempted to join the latter. The media could heighten that temptation by offering what Lincoln calls “disparity in spectacle.” Fringe exceptions like anti-lockdown protests and packed restaurants, she says, are more dramatic and telegenic than people responsibly staying at home, and so more likely to be covered. The risk is that rare acts of incaution will seem like normal behavior.
“There’s a natural saturation point for images of health systems in crisis,” Lincoln adds, and newly overwhelmed hospitals might be ignored in favor of fresher narratives. The local media are better positioned to pick up the nuances of a patchwork story, but of the counties that had reported cases of COVID-19 by early April, 37 percent had lost their local newspaper in the past 15 years. If the virus does indeed resurge and states need to shut down again, people may not comply, because they’ll be misinformed and distrustful.
A second future is also possible. “When this outbreak began in China, everyone said, Thank God it’s not here,” Jha says. “It moved to Western Europe and people said, They have government-run health care; that won’t happen here. Then it hit New York and Seattle, and people said, It’s the coasts. At every moment, it’s more tempting to define the other who is suffering, as opposed to seeing the commonalities we all share.” But as the virus spreads, Americans may run out of others to discriminate against. “Crises are political only until they are personal,” wrote the journalist Elaina Plott, in a piece about a Louisiana woman who convinced her conservative friends to take the coronavirus seriously after her own husband fell sick. Similarly, President Donald Trump’s claims that the virus will go away on its own will ring false to supporters who know someone fighting for breath.
There are signs that this is happening. While Trump’s popularity predictably surged during the crisis, his “rally around the flag” boost was a blip compared with the prolonged peaks of other leaders. Polls have also shown that pandemic partisanship is narrowing, with Democrats and Republicans more united in how seriously they view the threat. Beth Redbird, a sociologist at Northwestern University, has been surveying 200 people a day since mid-March, and “70 to 75 percent of people support most social-distancing measures,” she says. “Those are really large numbers in a society where 52 percent is often viewed as huge support. We rarely see that outside of authoritarian polling. Americans are by and large reading information in a very similar way.”
Economic indicators support this view. Even in conservative states, activity plummeted before leaders closed businesses, and hasn’t rebounded since restrictions were lifted. As such, Redbird doesn’t share the widely held fear that Americans have become inured to social distancing and will refuse to suffer through it again. The bigger risk, she says, is that demoralizing bouts of shutdowns and reopenings will nix any prospect of economic recovery. “You only get to say Go out, trust me once,” she says. “They won’t believe you the second time.”
Both possible futures are confounded by three aspects of COVID-19 that make the pandemic hard to grasp, and that are amplified by the patchwork effect. First, the disease progresses slowly. It seems to take an average of four or five days, and a maximum of 14, for an infected person to show symptoms. Those symptoms can take even longer to become severe enough for a hospital stay, and longer still to turn fatal. This means that new infections can take weeks to manifest in regional statistics. May’s declining cases are the result of April’s physical distancing, and the consequences of May’s reopenings won’t be felt until June at the earliest. This long gap between actions and their consequences makes it easy to learn the wrong lessons.
Read: Why some people get sicker than others
Second, the pandemic is shaped by many factors. Social distancing matters, but so do testing capacity, population density, age structure, wealth, societal collectivism, and luck. Many countries that successfully controlled the coronavirus used masks; New Zealand did not. Many had decisive leaders; Hong Kong did not. It is easy to look at a patchwork and create just-so stories about why one place succumbed while another triumphed. But no single factor can explain differences across nations or regions.
Third, the disease spreads unevenly. Some cases infect no one, and others infect many. In Washington State, a choir member infected 51 fellow singers during a few hours of rehearsal. In Ghana, a worker in a fish factory infected 533 colleagues. These “super-spreader events,” which are rare but pivotal, become especially important when cases dip. They mean that an untroubled region may continue that way for some time, but that once cases start growing, they can really grow.
If a state reopens and sees no immediate spike in cases, is that because it was justified, because insufficient time has passed, because other things went right, or because unlucky super-spreader events haven’t yet happened? In a patchwork, these questions will be asked millions of times over, and many answers will be wrong.
The COVID-19 pandemic is not a hurricane or some other disaster that will come and go, signaling an obvious moment when recovery can begin. It is not like the epidemics of fiction, which get worse until, after some medical breakthrough, they get better. It is messier, patchier, and thus harder to predict, control, or understand. “We’re in that zone that we don’t see movies made about,” says Lindsay Wiley, a professor of public-health law at American University.
II. The Patchwork Response
A patchwork was inevitable, especially when a pandemic unfolds over a nation as large as the U.S. But the White House has intensified it by devolving responsibility to the states. There is some sense to that. American public health works at a local level, delivered by more than 3,000 departments that serve specific cities, counties, tribes, and states. This decentralized system is a strength: An epidemiologist in rural Minnesota knows the needs and vulnerabilities of her community better than a federal official in Washington, D.C.
But in a pandemic, the actions of 50 uncoordinated states will be less than the sum of their parts. Only the federal government has pockets deep enough to fund the extraordinary public-health effort now needed. Only it can coordinate the production of medical supplies to avoid local supply-chain choke points, and then ensure that said supplies are distributed according to need, rather than influence. Instead, Trump has repeatedly told governors to procure their own tests and medical supplies.
Read: Trump is putting himself at risk for COVID-19
Michael Kilkenny of the Cabell-Huntington Health Department, in West Virginia, says his state found itself short on swabs, disinfectant, and protective equipment; unable to compete in the global market; and abandoned by the White House. “It felt terrible,” he says. “We’ve been making homemade masks, or using bleach solutions. We had to fend for ourselves.” While reporting on pandemics in the Democratic Republic of Congo in 2018, I heard health-care workers repeatedly joke that the 15th article of the country’s constitution is “Débrouillez-vous”—French for “Figure it out yourself.” It’s a droll resignation that when resources are scarce, the government won’t fix your problems, and it’s on you to make do. The U.S., a country that’s more than 400 times wealthier, has seemingly adopted “Débrouillez-vous” as national policy.
Even health officials in well-off states aren’t comfortable with a situation in which preparedness has more to do with wealth and connections than need. “We have everything we need,” says Angela Dunn, the state epidemiologist for Utah, where Governor Gary Herbert moved quickly to buy and secure tests and supplies. “But we did it in a very capitalistic way, and that’s not the best way to deal with a pandemic.” States have tried to level the playing field on their own. Wyoming ended up with few cases but a glut of testing reagents, which it provided to Colorado and Utah when those states saw spikes, Dunn says. “There’s a small barter system, but it’s not sustainable and it doesn’t work at scale,” she says. “I don’t know if Colorado is lacking supplies. If they have a huge spike, that’ll impact Utah. It’s in our interests to make sure everyone’s protected, and without federal coordination, that’s hard to do.”
In some cases, the federal government has actively undermined the states. Charlie Baker, the Republican governor of Massachusetts, tried to buy protective equipment, but was thrice outbid by the federal government; he ended up using the New England Patriots’ jet to fly 1.2 million masks over from China, many of which turned out to be faulty. When Larry Hogan, Maryland’s Republican governor, procured 500,000 tests from South Korea, he kept them guarded in an undisclosed location so they wouldn’t be seized by the feds. This is not federalism working as intended, where different tiers of government work together. Instead of devolving control to the states, the Trump administration has ceded the U.S. to the virus.
The U.S. now heads into summer only slightly more prepared to handle the pandemic that cost it so dearly in the spring. According to the COVID Tracking Project at The Atlantic, the U.S. is now testing 366,000 people a day—a record high. But experts estimate that the country needs 500,000 to several million daily tests. Here, too, a patchwork is apparent. An analysis by NPR and Harvard’s Global Health Institute showed that in early May, only nine states were doing sufficient testing, and another 31 weren’t even halfway to their requisite threshold.
“I would have hoped for more, considering the cost of that time,” says Natalie Dean, a statistician at the University of Florida. Stay-at-home orders were necessary but ruinous, economically and emotionally. Their purpose was to buy time for the country to catch its breath, steel its hospitals, and roll out a public-health plan capable of quashing the virus. Many such plans exist. Umpteen think tanks and academics have produced their own road maps for dialing society back up. These vary in their details, but are united in at least having some. By contrast, the Trump administration’s guidelines for “opening up America again” are so bereft of operational specifics that they’re like a cake recipe that simply reads, “Make cake.”
The Centers for Disease Control and Prevention prepared a more detailed guide but was blocked from releasing it by the White House, according to an Associated Press report. The guidance it has released seems carefully worded to avoid the term guidelines, as if it’s “trying to fly under the radar,” Wiley says. “The abdication of federal responsibility has left states with little choice but to ease the most disruptive physical-distancing measures without the testing data that would make us more confident that cases won’t rapidly surge.” (The CDC finally and quietly released a slightly abridged version of its fuller report on Tuesday.)
Read: There’s one big reason the U.S. economy can’t reopen
The Trump administration “isn’t known for consistency of messaging, so we’ll never put our full faith in that,” says Kilkenny of West Virginia. “We pretty much ran our own state here.” At the time of this writing, only five states and the District of Columbia are still under some form of lockdown. A few, such as Alaska, Hawaii, and Montana, eased restrictions after their caseloads had fallen to low single digits. Idaho is reopening cautiously, despite being one of the less affected states.
Georgia went all in on April 24, reopening gyms, restaurants, theaters, salons, and bowling alleys at a point when it had five of the 10 counties with the highest COVID-19 death rates nationwide, and was testing just a fifth as many people as it needed to. By contrast, Utah revived businesses a week later, when it had more than enough tests for everyone with symptoms, all their contacts, high-risk groups, and even random slices of the populace. Still, Dunn, the state epidemiologist, is nervous. “If we could stick it out for even a couple more months of stricter social distancing, it would do us a world of benefit,” she says. “There are embers everywhere, and they could ignite any moment.” Some states never put their fires out at all: Texas, Alabama, Kansas, Arizona, Mississippi, North Carolina, Wisconsin, and others all reopened while cases were still rising.
“It’s inevitable that we’ll see stark increases in infections in the next weeks,” says Oscar Alleyne of the National Association of County and City Health Officials. The experiences of other countries support that view. Success stories like South Korea, China, Singapore, and Lebanon all had to renew or extend social-distancing measures to deal with new bursts of cases. And they had all restrained the virus to a much greater extent than the U.S., which despite having just 4 percent of the world’s population has 31 percent of its confirmed COVID-19 cases (1.5 million) and 28 percent of its confirmed deaths (92,000).
In a connected country, flare-ups that begin in reckless states can easily spread into more cautious ones. Cellphone data, for example, reveal that after Georgia businesses revved back into action, more than 60,000 extra visitors poured in from neighboring states every day. Genetic studies show the risks of such movements. By using patterns of mutations to reconstruct the pandemic’s path, researchers have shown that most of New York’s cases likely stemmed from one introduction from Europe in mid-February. Most of Louisiana’s cases arose from just a couple of introductions from within the U.S. Just a few travelers can spark substantial outbreaks in new places.
To mitigate such risks, about two dozen states have asked out-of-town arrivals to self-quarantine for 14 days. But tighter restrictions would be a logistical and legal nightmare. States can regulate what happens within their borders, but have limited powers to control travel across them. Congress could potentially do so, but it’s unclear if the courts would uphold any restrictions. The right to travel is supported by Supreme Court precedents, but in 1965, the Court ruled that said right “does not mean that areas ravaged by flood, fire or pestilence cannot be quarantined” if unlimited travel would jeopardize the safety of the nation.
Anne Applebaum: The rest of the world is laughing at Trump
Legality aside, domestic-travel bans are of limited use. Even China’s extraordinary quarantine of Wuhan merely delayed the virus from reaching other parts of the mainland by three to five days. Much like social distancing, such measures only buy time. The better strategy is not to try and prevent the virus from traveling, but to build a public-health system nimble enough to catch it when it arrives. Don’t build one big wall; instead, ready a thousand nets.
In this, the U.S. is also behind. Prevented health threats are less visible than present ones, which means that successful public-health departments tragically make the case for their own diminishment. Since 2008, underfunded local departments have lost more than 50,000 jobs. Even now, Cincinnati’s health department has furloughed 36 percent of its staff. “How can you have a system that’s meant to be at the front line of the defense while it’s losing the staff it needs?” Alleyne asks.
Some states are trying to make up for these losses by hiring battalions of contact tracers. These people will call every infected person, talk through their needs, ask for names of anyone they’ve had close or prolonged contact with in the past two days, and call those contacts, too. The process isn’t complicated, but it is laborious. Experts have estimated that the U.S. needs 100,000 to 300,000 contact tracers, and the nation has been slow to recruit them. Selena Simmons-Duffin of NPR reported that only North Dakota had recruited enough as of May 7, although six more states and the District of Columbia were set to.
Things are improving, though. When Danielle Allen of Harvard canvassed several mayors in mid-April, they weren’t taking contact tracing seriously. When she spoke with them again in May, “they were on top of it,” she says. “I was blown away by how much changed in three weeks.” New York State alone is planning to hire 6,000 to 17,000 contact tracers, while California is aiming for 20,000. “This really is the best tool we have to manage the pandemic until we have a safe and effective vaccine,” says Crystal Watson at the Johns Hopkins Center for Health Security.
Will this system, combined with mask wearing and hand-washing, be enough to contain a patchwork pandemic? Complicating matters, people with COVID-19 can spread the coronavirus before showing symptoms. And yet, that hasn’t fazed other countries. South Korea has been rightly praised for its success, and though one nightclub-goer recently sparked a surge of at least 168 cases, the country seems to have contained this new outbreak too. Basic public-health measures have similarly worked in countries as diverse as Iceland, Jordan, Singapore, Germany, and New Zealand. And they have suppressed epidemics of the past, from smallpox in the 19th century to Ebola in 2014. “Some silver bullet isn’t going to save us. We can save ourselves,” says Gregg Gonsalves, an epidemiologist at Yale. “We have very old-school tools that beat fucking smallpox.”
Derek Thompson: The technology that could free America from quarantine
But those very old-school tools must also contend with old-school problems, which are difficult to recognize, let alone beat.
III. The Patchwork Legacy
The current patchwork is not random. Nor is it solely the consequence of America’s actions in 2020. It has emerged from a much older, deeper patchwork.
U.S. policies that evicted Native Americans from their own lands have long left indigenous peoples with insufficient shelter, water, and resources, making them vulnerable to infectious diseases like smallpox, cholera, malaria, dysentery, and now COVID-19. Up to 40 percent of the 170,000-person Navajo (Diné) Nation have no running water; they can’t effectively wash their hands. About 30 percent have no power; they burn coal or wood for heat, resulting in irritated lungs that are vulnerable to a respiratory pandemic—a problem exacerbated by uranium mining on their lands. Chronic underfunding has saddled them with crowded living conditions through which the virus easily spreads, dispersed health-care facilities that are low on beds and ventilators, and high rates of chronic conditions that increase the odds of dying from COVID-19. “The lack of basic services on the reservation isn’t due to our choosing to live this way,” wrote Wahleah Johns, a Diné woman, in The New York Times. “It’s because treaties and federal policies dictate how we live.”
Thanks to traumas that accrued over generations and stressors that accrue over individual lives, the Navajo Nation has more per capita cases of COVID-19 than any U.S. state and nine times as many per capita deaths as neighboring Arizona. While Arizona has loosened its distancing restrictions, the Navajo Nation has been forced to tighten its orders.
Black Americans have fared little better. After the Civil War, white leaders deliberately kept health care away from black communities. For decades, former slave states wielded political influence to exclude black workers from the social safety net, or to ensure that the new wave of southern hospitals would avoid black communities, reject black doctors, and segregate black patients. “Federal health-care policy was designed, both implicitly and explicitly, to exclude black Americans,” wrote the journalist Jeneen Interlandi for The New York Times’ 1619 Project.
Ibram X. Kendi: Stop blaming black people for dying of the coronavirus
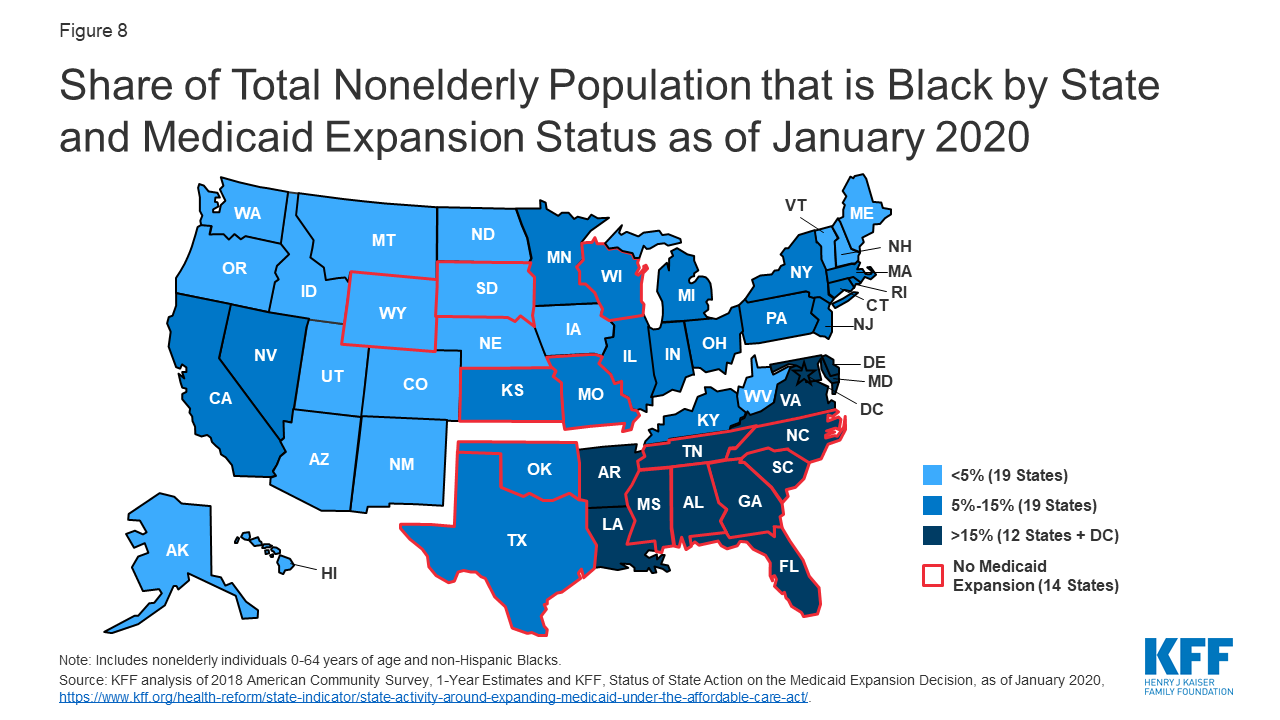
This is one reason why the U.S. still relies on employer-based insurance, which black people have always struggled to access. Such a system “was the only fit for a modernizing society that could not abide black citizens sharing in societal benefits,” wrote my colleague Vann Newkirk II. Over the past century, every move toward universal health care, and thus toward narrower racial inequities, was fiercely opposed. The Affordable Care Act, which almost halved the proportion of uninsured black Americans below the age of 65, was most strongly fought by several states with large proportions of black citizens.
{kind=link}
Last year, when the Global Health Security Index graded every country on its pandemic preparedness, the United States had the highest overall score, 83.5. But on access to health care specifically, it scored just 25.3. (Out of 195 countries, it tied with The Gambia for 175th place.) That is at least partly the consequence of letting segregationist tenets influence the allocation of health care. “The resulting arrangement all but guarantees an inadequate national response to a national crisis,” wrote Amy Kapczynski and Gregg Gonsalves of Yale.
In almost every state, COVID-19 disproportionately infects and kills people of color—a pattern that Ibram X. Kendi has called “a racial pandemic within the viral pandemic.” Pundits have been quick to blame poor health or unsafe choices, without considering the roots of either. Racism in policing means that many black people don’t feel safe wearing the masks that would protect their neighbors. Racism in medicine means that black patients receive poorer health-care than white ones. Racism in policy has left black neighborhoods with less healthy food and more pollution, and black bodies with higher rates of diabetes, heart disease, stress, and what the demographer Arline Geronimus calls “weathering”—poor health that results from a lifetime of discrimination and disadvantage. “When America catches a cold, black people get the flu,” says Rashawn Ray, a sociologist at the University of Maryland. “In 2020, when America catches COVID-19, black people die.”
These inequities will likely widen. Even before the pandemic, inequalities in poverty and access to health care “were concentrated in southern parts of the country, and in states that are politically red,” says Tiffany Joseph, a sociologist at Northeastern University. Not coincidentally, she says, those same states have tended to take social-distancing measures less seriously and reopen earlier. The price of those decisions will be disproportionately paid by black people.
Adam Serwer: The coronavirus was an emergency until Trump found out who was dying
Vulnerability to COVID-19 isn’t just about frequently discussed biological factors like being old; it’s also about infrequently discussed social ones. If people don’t have health insurance, or can afford to live only in areas with poorly funded hospitals, they cannot fight off the virus as those with more advantages can. If people work in poor-paying jobs that can’t be done remotely, have to commute by public transportation, or live in crowded homes, they cannot protect themselves from infection as those with more privilege can.
These social factors explain why the idea of “cocooning” vulnerable populations while the rest of society proceeds as normal is facile. That cocooning already exists, and it is a bug of the system, not a feature. Entire groups of people have been pushed to the fringes of society and jammed into potential hot zones. Of the 100 largest clusters of COVID-19 in the U.S., nearly all have occurred in prisons, meatpacking plants, nursing homes, and psychiatric or developmental-care facilities. (The only exceptions are a naval vessel and three power plants; the infamous Grand Princess cruise is only No. 148 on the list.)
These places, along with homeless shelters and immigrant detention centers, are hubs for outbreaks that can easily spread to the surrounding communities. Prisons and nursing homes have staff and visitors who live in nearby towns. Large prisons, in particular, are usually situated in rural areas with small community hospitals that can be easily overrun by an outbreak. And many employees in nursing homes and meatpacking plants are immigrants who care for the nation’s elderly and process its steaks while also being cut off from health care by the Trump administration’s policies. They are both more likely to get sick, and less likely to get better.
This point cannot be overstated: The pandemic patchwork exists because the U.S. is a patchwork to its core. New outbreaks will continue to flare and fester unless the country makes a serious effort to protect its most vulnerable citizens, recognizing that their risk is the result of societal failures, not personal ones. “People say you can’t fix the U.S. health system overnight, but if we’re not fixing these underlying problems, we won’t get out of this,” says Sheila Davis of Partners in Health. “We’ll just keep getting pop-ups.”
Leaders can specifically place testing sites in poor, black, and brown communities, rather than the rich, white areas where they tend to be concentrated. New York Governor Andrew Cuomo, for example, is turning 24 churches in low-income areas into testing centers, while Maryland Governor Larry Hogan placed a testing facility in the heart of the predominantly black Prince George’s County. Officials can remove people from risky environments: Leann Bertsch, who directs the North Dakota Department of Corrections, has argued that prisoners should be freed if they are over 50, have serious illnesses, or are within two years of parole or release. A bipartisan group of 14 senators has made a similar call for decarceration.
Policies can also support people in protecting themselves. Essential workers earn low hourly wages and cannot afford to miss a shift, even if they have symptoms. “The only way to prevent them from going to work is to give them paid sick leave,” Ray says. The same goes for a minimum living wage, hazard pay, universal health care, stipends for people who are self-isolating, debt moratoriums, rent freezes, food assistance, and services to connect people with existing support.
The pandemic discourse has been dominated by medical countermeasures like antibody tests (which are currently too unreliable), drugs (which are not cure-alls), and vaccines (which are almost certainly at least a year away). But social solutions like paid sick leave, which two in three low-wage workers do not have, can be implemented immediately. Imagine if the energy that went into debating the merits of hydroxychloroquine went into ensuring hazard pay, or if the president, instead of wondering out loud if disinfectant could be injected into the body, advocated for health care for all? “We have decades of social-science research that tells us these things work,” says Courtney Boen, a sociologist at the University of Pennsylvania. “It’s a question of political will, not scientific discovery.”
And while a vaccine will protect against only COVID-19 (if people agree to take it at all), social interventions will protect against the countless diseases that may emerge in the future, along with chronic illnesses, maternal mortality, and other causes of poor health. “This pandemic won’t be the last health crisis the U.S. faces,” Boen says. “If we want to be on better footing the next time, we want to reduce the things that put people at risk of being at risk.”
Of all the threats we know, the COVID-19 pandemic is most like a very rapid version of climate change—global in its scope, erratic in its unfolding, and unequal in its distribution. And like climate change, there is no easy fix. Our choices are to remake society or let it be remade, to smooth the patchworks old and new or let them fray even further.

Source link